

RAPID Respiratory Acceleration Pathway for Identification & Diagnosis
Accelerating Respiratory diagnosis following emergency department or urgent care discharge.
Status: Seeking Founding Sponsors
The Challenge
Patients with chronic obstructive pulmonary disease (COPD) are frequently diagnosed late-often after repeated Emergency Department (ED) visits for acute respiratory events. Up to 70% -80% of cases remain undiagnosed, and symptoms may persist for years prior to diagnosis.
The gap is largely attributed to gaps in coordination at care transition points. Patients presenting to the ED with bronchospasm, wheezing, or acute symptoms are typically stabilized and discharged without confirmed diagnosis or coordinated follow-up. Spirometry, required for diagnosis, is rarely performed in acute settings and is often deferred.
As a result:
COPD drives ~1.5–1.8M ED visits annually—a high-volume but underutilized entry point for diagnosis
Patients treated for bronchospasm are discharged without being routed into a COPD diagnostic pathway
Published evidence demonstrates systematic leakage across this pathway, particularly at ED discharge and follow-up
Capturing this moment enables earlier diagnosis, faster treatment initiation, and improved patient access
The opportunity is not to generate new evidence, but to align Emergency Medicine and Pulmonology around a coordinated diagnostic pathway at discharge. By enabling early identification, structured follow-up, and rapid access to specialist evaluation and testing, it becomes possible to accelerate diagnosis, initiate appropriate therapy sooner, and reduce avoidable utilization.
The challenge is not clinical capability-it is designing a scalable model that connects ED care, pulmonology evaluation, and patient insight into a seamless pathway.
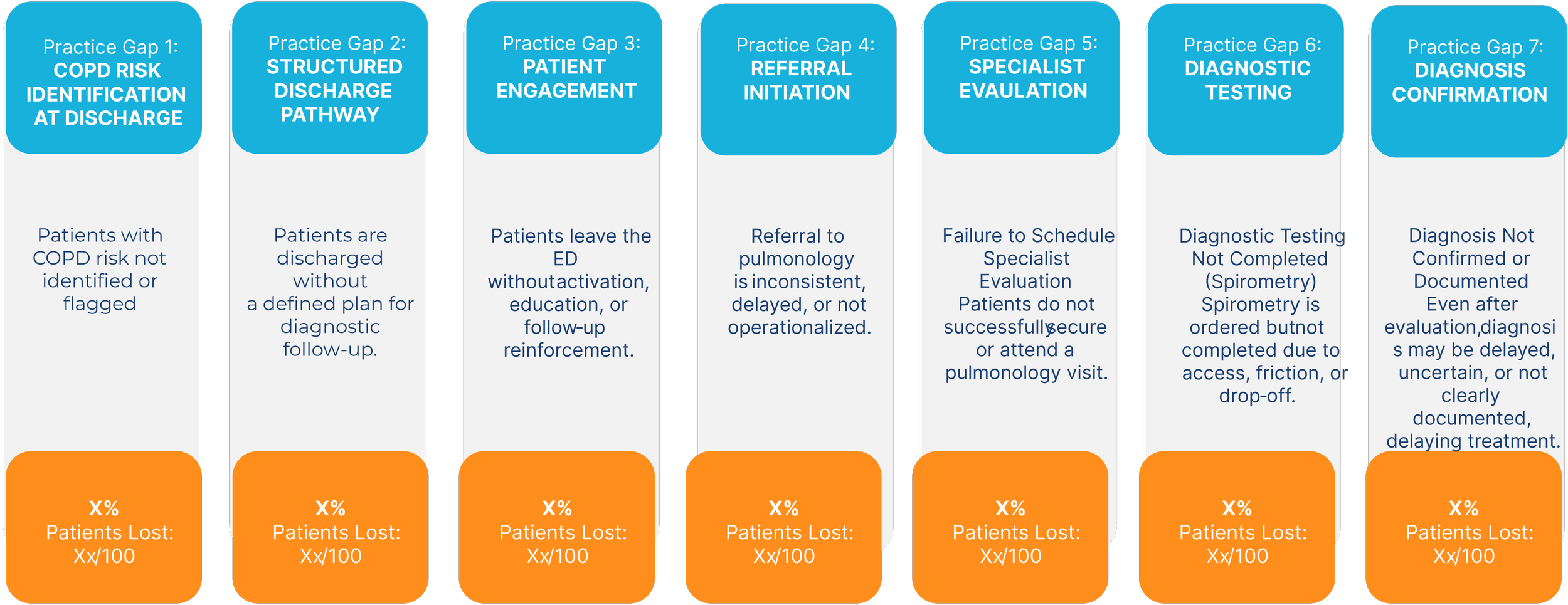
Illustrative model demonstrating cumulative patient leakage across the ED-to-diagnosis pathway, based on published evidence of underdiagnosis, discharge without follow-up, and delayed access to specialty care
The Opportunity
The opportunity is not to generate new evidence, but to align Emergency Medicine and Pulmonology around a coordinated diagnostic pathway at discharge.
The RAPID Model
Designing a coordinated pathway from ED discharge to diagnosis.
Focus & Scope
RAPID will define and validate a scalable model for accelerating COPD identification and diagnosis following Emergency Department (ED) discharge.
During Phase I, participants will work collaboratively to:
Define Patient Identification Criteria
Establish practical criteria for identifying patients with suspected COPD at ED discharge based on presenting symptoms, treatment patterns, and clinical history.
Establish a Coordinated Referral Pathway
Design a structured process that connects eligible patients from the ED to timely pulmonology evaluation and follow-up care.
Create a Patient Engagement Model
Develop approaches to support patient activation, continuity, and participation during the transition from acute care to specialty evaluation.
Operationalize Pulmonology Access
Define workflows that enable rapid specialist access, including traditional referral models, telehealth-enabled pathways, and other scalable approaches.
Define the Diagnostic Workflow
Establish a coordinated approach for completing diagnostic evaluation, including pulmonary function testing, imaging, and specialist assessment.
Establish a Measurement Framework
Define key performance indicators and implementation measures to evaluate pathway effectiveness, including follow-up completion, time to diagnosis, treatment initiation, and healthcare utilization.
The objective of Phase I is to produce a practical, implementable model that can be evaluated, refined, and expanded across additional healthcare settings.
Phase 1 Outputs
Phase I will produce a set of practical implementation assets designed to support earlier COPD identification, improved care coordination, and scalable adoption across healthcare settings.
ED-to-Pulmonology Care Pathway Model
A defined operational model outlining how patients are identified, referred, evaluated, and diagnosed following Emergency Department discharge, including key coordination points across care settings.
Patient Identification & Engagement Framework
A structured framework for identifying high-risk patients and supporting engagement, follow-up, and continuity during the transition from acute care to specialty evaluation.
Rapid Referral & Diagnostic Workflow
A coordinated workflow designed to accelerate specialist access and diagnostic evaluation, including referral processes, intake pathways, pulmonary function testing, imaging, and clinical assessment.
Performance Measurement Framework
A standardized set of implementation and outcome measures used to evaluate pathway effectiveness, including follow-up completion, time to diagnosis, treatment initiation, patient engagement, and healthcare utilization.
Implementation Playbook
A practical guide outlining operational requirements, workflow integration considerations, stakeholder roles, and lessons learned to support replication and scale across additional sites and health systems.
Sponsorship Opportunity
RAPID is being developed through a multi-stakeholder implementation model that brings together health systems, clinicians, patient organizations, and industry partners to address a shared challenge: accelerating COPD identification and diagnosis following Emergency Department discharge.
Sponsors support the initiative through participation, practical input, and shared learning while AHIS maintains independent governance and editorial oversight.
Founding Sponsor
Founding Sponsors play a leadership role in the development of the initiative and help inform program priorities and implementation strategy.
Benefits include:
Participation in initiative design and working sessions
Participation in pathway validation discussions
Early visibility into pilot performance and emerging insights
Executive synthesis briefings and leadership updates
Recognition as a Founding Sponsor (unless anonymity requested)
First consideration for participation in future expansion phases
Contributing Sponsor
Contributing Sponsors participate in the initiative and support the development and refinement of the care pathway model.
Benefits include:
Participation in working sessions
Participation in pathway validation discussions
Executive synthesis briefings
Access to pilot outputs and summary insights
Recognition as a Contributing Sponsor (unless anonymity requested)
Supporting Sponsor
Supporting Sponsors help advance the initiative and gain visibility into resulting frameworks, tools, and learnings.
Benefits include:
Access to final pilot outputs
Access to implementation summaries and key learnings
Recognition as a Supporting Sponsor (unless anonymity requested)
Participation Principles
To preserve the integrity and independence of the initiative:
Sponsorship does not confer governance authority
Sponsors do not receive editorial control over outputs
Participation is non-voting
Individual patient or health system data are not shared
AHIS retains final editorial authority over all publications, frameworks, and deliverables
All participants contribute to a collaborative implementation effort designed to improve real-world care delivery and accelerate adoption of evidence-based practices.
Join RAPID
Help design a scalable model for accelerating Respiratory diagnosis following emergency department discharge.
Operationalizing Tele-ICUAcross Safety-Net Hospitals
It All Begins Here
Location: Urban Detroit, MI Focus: Culturally Competent Preventive Care
The Challenge
High rates of Type 2 Diabetes in specific Detroit neighborhoods were compounded by "food deserts" and a historical distrust of traditional clinical institutions. Existing clinical DPPs saw a 60% dropout rate within the first three months.
The Intervention
Faith-Based Integration: Partnering with 12 local churches to host "Wellness Sundays."
Peer Educators: Training "Health Ambassadors" from within the congregation to lead nutrition workshops and walking groups.
The "Green Grocery" Voucher: A partnership with local markets to provide subsidies for fresh produce, tied to program attendance.
Key Outcomes
85% Retention Rate: Leveraging the social fabric of the church led to significantly higher engagement.
Weight Loss: Participants averaged a 5.5% reduction in body weight over 12 months.
Clinical Marker: Average A1c levels dropped from 6.2% to 5.8% across the cohort.